
Case Studies That Can Make Public Health More Practical
Eleven real-world cases that teach what textbooks can't


A pregnant waitress, Martinah Payne-Yehuda, testified to the New York City Council in 2002 and described what it was like to breathe other people’s cigarette smoke for eight hours a night. She wasn’t an epidemiologist. She didn’t cite relative risks. She told the Council what her workday felt like.
Because of her testimony and others stories like it, the Smoke-Free Air Act passed. Opponents predicted the restaurant industry would collapse. It didn’t. Restaurant business increased. During the next decade, adult smoking in New York City decreased 28% and youth smoking dropped 52%.
When the City Council speaker demanded exemptions for smoking rooms, the health department didn’t fight the exemption. Instead, they wrote engineering specifications so technically demanding that no bar could afford to build one. Two investigated and neither proceeded.
That kind of strategy is rarely taught in classrooms
The NYC Smoke-Free case is one of eleven case studies now available for free as part of the teaching materials for The Formula for Better Health. Each comes with a student handout, instructor guide, test bank, and answer key. Faculty can build a semester-long course, use individual chapter guides, or drop a single case into an existing class. An interactive version of the case studies is under construction.
Last week, I discussed how public health training can close the gap between knowing what works and making it happen. This week, I’m focusing on why specific case studies make a big difference.
What makes these cases stand out
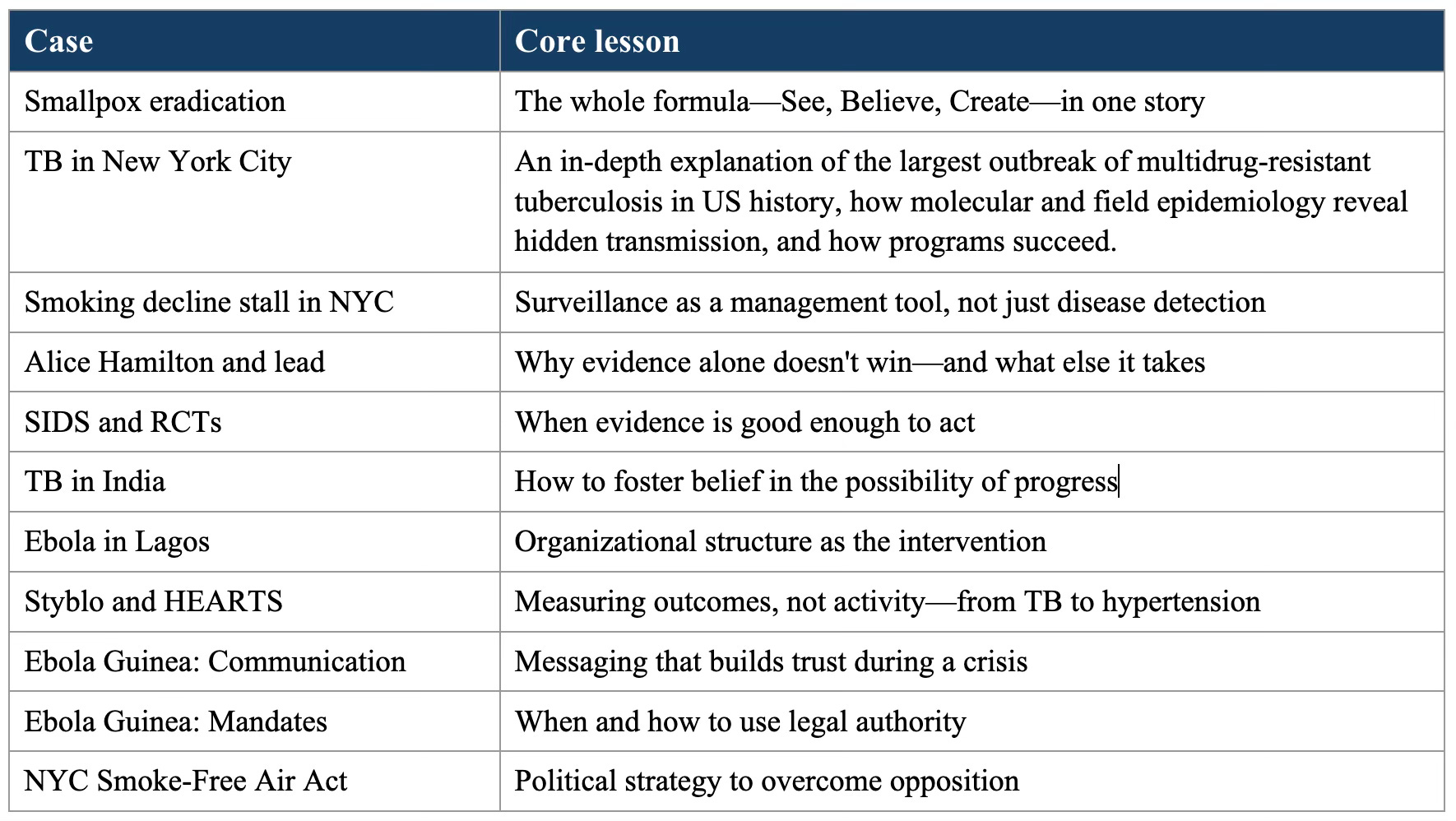
Most case studies describe what happened. These put students at decision points and ask: What would you do? Instructor materials provide a sequence of the material so students face the same uncertainty practitioners faced. Here are a few examples, with the full set in the table below.
Alice Hamilton and the Cassandra curse. Hamilton documented lead poisoning for decades. The 1925 Surgeon General’s conference was stacked with industry-affiliated scientists. Their conclusion was that more study was needed. The case identifies six drivers that keep dangerous products on the market despite clear evidence of harm. Students map those drivers onto a contemporary problem of their choice. Which are operating? Where’s the money? Whose story gets heard?
Styblo and HEARTS. Karel Styblo’s single rule for tuberculosis control was: “No cheating. Every patient in your area, you are responsible for their outcome.” This rule transformed how programs are measured. Most programs count patients enrolled, but Styblo counted patients cured to reveal whether a program is working. Students apply Styblo’s question to a program of their own choosing and design the simplest possible monitoring system for a resource-constrained setting. The lesson: Simplicity is a design principle, not a compromise.
SIDS and the best available evidence. Dr. Ed Mitchell found a pattern in infant deaths—many had been placed prone to sleep. A statistician confirmed on the back of an envelope that prone sleeping accounted for most deaths from Sudden Infant Death Syndrome (SIDS). Mitchell’s reaction: “I couldn’t believe something as simple as placing babies prone could increase the risk of sudden death substantially. Basically thought it was rubbish.” No RCT was ever done and none was needed – and none could have been done, practically and ethically. New Zealand launched a Back to Sleep campaign based on observational evidence and SIDS deaths plummeted. The case drives home a critical lesson: RCTs are not the gold standard for every question. The best decisions come from the best available evidence appropriate to the question being studied.
What students do with these cases
These cases ask students to do what practitioners do. Design a surveillance system. Apply a political strategy framework to a real policy fight. Diagnose why a program is failing. Build a monitoring system simple enough to work. Map the forces that prevent action on a problem they care about.
Every case applies to CEPH foundational competencies. The instructor guides include detailed teaching prompts. The test banks assess applied reasoning, not just recall. Several cases include slide decks.
Free and ready to use
The materials are free. Click here to access.
At a World Health Organization meeting on TB evaluation, a participant dismissed the insistence on measuring cure rates: “Oh, you’re one of those ‘outcome‘ people.” These case studies are for the outcome people — and for training the next generation to become them.
