
Epidemics Aren't Inevitable. We Can Prevent and Stop Them.
As an alarming new Ebola outbreak spreads, these stories offer important lessons


Most disease outbreaks never make the news because front line health and public health workers caught them before they spiraled into major health emergencies.
A health worker notices something wrong. A surveillance system flags an unusual cluster. A response team moves fast, and a crisis that could have spiraled into tragedy...doesn’t. These quiet victories are invisible, but they carry lessons we can’t afford to ignore.
This week, as an alarming Ebola outbreak in the Democratic Republic of the Congo spreads, Resolve to Save Lives released our latest Epidemics That Didn’t Happen report.
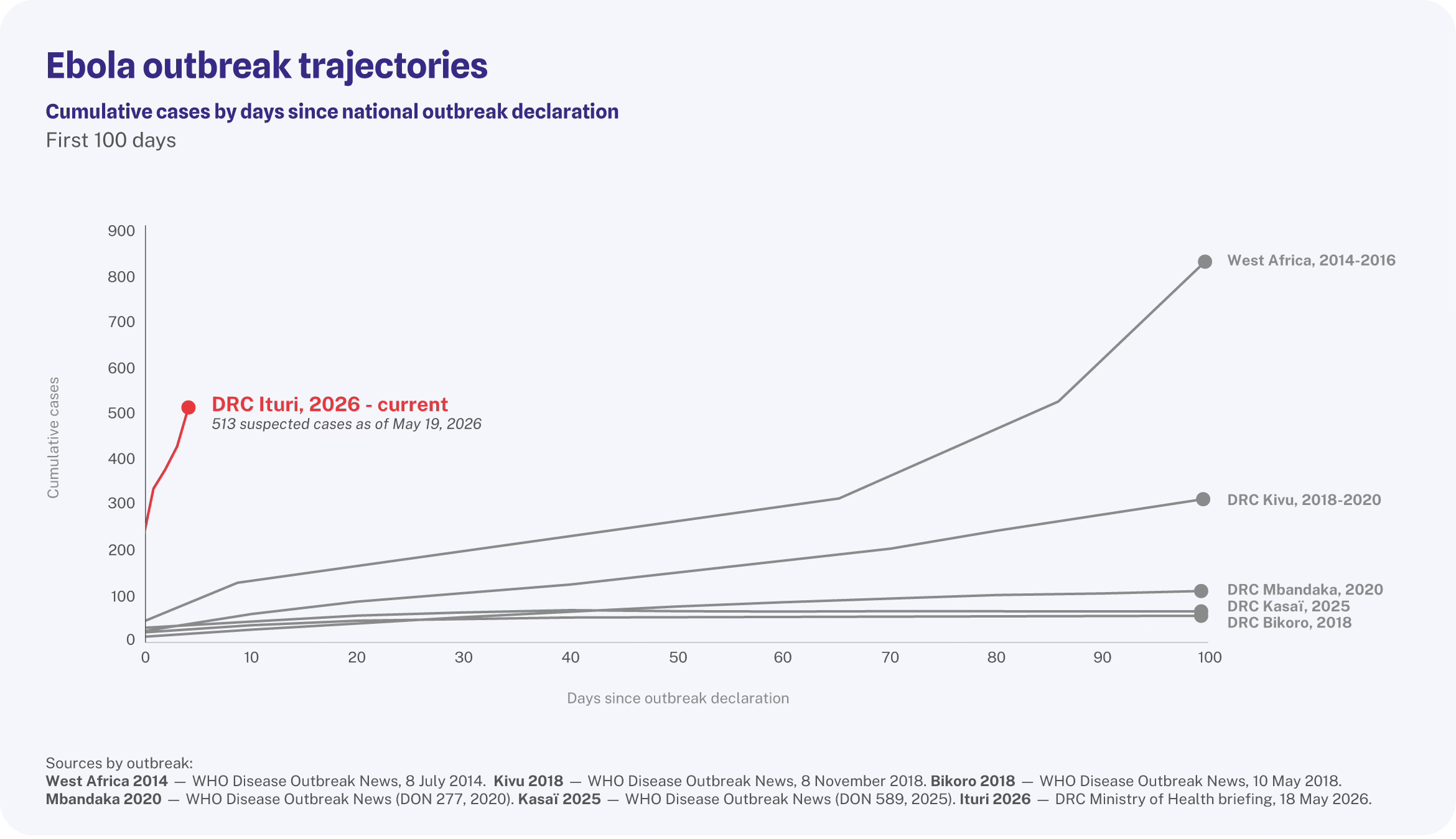
The Ebola outbreak is a devastating illustration of the cost of delayed detection. The virus likely spread undetected for months, and by the time it was confirmed and response activities began, the virus had a running start. There were nearly 10 times this many cases in this outbreak as there were at the same time of the catastrophic 2014 West Africa epidemic. It is spreading in a region where healthcare is already stretched and underfunded. The WHO has declared a Public Health Emergency of International Concern. There’s no approved vaccine and no proven antiviral treatment, although supportive medical care can greatly increase the likelihood that patients survive.
Every day of delay increases the risk to lives and livelihoods. That’s why the stories in this year’s Epidemics That Didn’t Happen report matter. They show what happens when countries get detection and response right—and why the world, including the United States, must stay engaged in building and maintaining the systems that make it possible.
Uganda is an excellent example. In 2022, an Ebola outbreak in Uganda killed 55 people. A new outbreak last year was contained with far fewer deaths (four). What changed? Speed. Between the two outbreaks, Uganda built faster systems for detection and response, guided by the 7-1-7 target: detect within 7 days of emergence, notify public health authorities within 1 day, establish all essential control measures within 7 days of notification. The 7-1-7 approach gave Uganda the opportunity to learn from the first outbreak and close gaps in preparedness. As another ebolavirus threatens the country again, Uganda is better prepared.
The other stories in this year’s report also offer powerful lessons. South Sudan deployed a response team faster than ever and stopped a cholera outbreak before it claimed a single life. El Salvador diagnosed malaria cases early enough to protect its malaria-free status and its population. The Caribbean Public Health Agency used a new digital surveillance system during the Cricket World Cup to protect millions of residents and visitors from outbreaks that never took hold. These stories are the result of systems built before crises hit.
These successes share two things: fast detection and fast response. Finding and responding to an outbreak within the 7-1-7 window can make the difference between a small disease outbreak and an epidemic. Having response teams ready to move, without waiting weeks for approvals or resources, can break chains of transmission. Strong primary health care, real-time reporting, and cross-border coordination allow countries to see threats early.
The DRC outbreak shows what’s at stake when those systems fall short. The stories in our Epidemics That Didn’t Happen report show what’s possible when they work. The gap between those two outcomes is a choice—one that countries, donors, and global health leaders make long before any outbreak begins.
These stories deserve to be more widely known. Please read the report and share it. Epidemics aren’t inevitable. We know how to stop them. The proof is in the outbreaks you never heard about.