
What Disease Detectives Actually Do
Inside the work of minimizing spread and maximizing survival


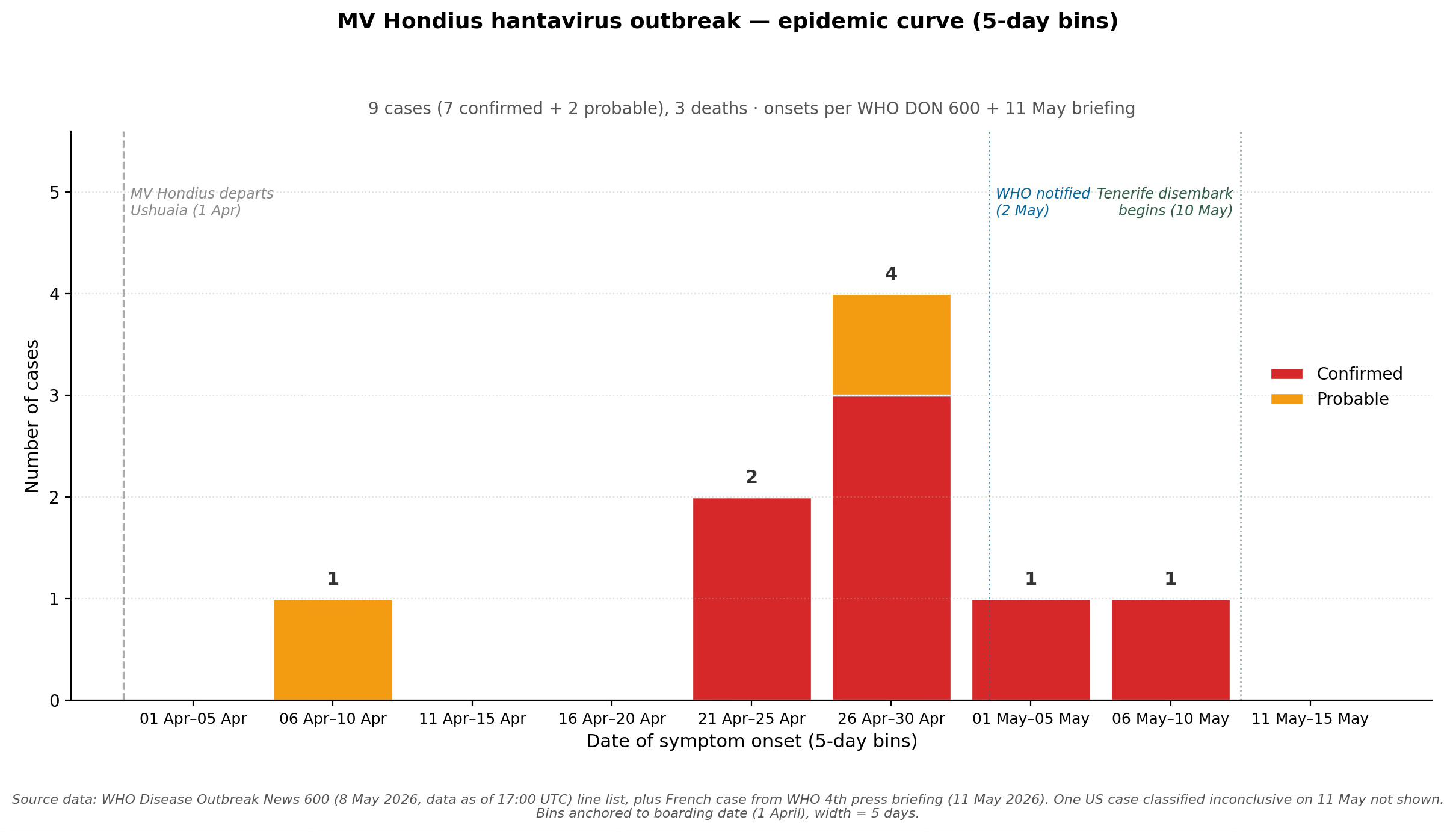
By the time disease detectives caught up with the MV Hondius, the ship was a floating outbreak.
It had left Ushuaia, at the southern tip of South America, on April 1, bound for Antarctica—about 600 miles south across the Drake Passage—and back. Ten days out, a 70-year-old Dutch passenger died on board from what looked like a respiratory illness. No specimens were taken. The body remained on board. The ship sailed on.
Two weeks after that, his widow, on her way home through Johannesburg, collapsed at the airport and died in hospital there.
On May 2, a lab at South Africa’s National Institute for Communicable Diseases identified Andes hantavirus by PCR in samples from a British passenger evacuated from Ascension Island. The same lab soon confirmed it in stored samples from the widow.
Epidemiologists are disease detectives. Investigations like this are what they live for. As I wrote in The Formula for Better Health, “A police detective can solve a murder; a disease detective can save thousands or even millions of lives by solving an epidemiologic mystery.”
The first step is to establish a case definition. A case definition has three elements: person, place, and time. Who could be infected (passengers and crew of the MV Hondius). Where (the ship and, potentially, its ports of call). When (symptom onset between specific dates). Get this wrong and you either miss cases or patterns. WHO published the Hondius case definition on May 8, with three tiers—suspected, probable, confirmed—and operational thresholds for each. That document is the spine of the response. Once there’s a case definition, detectives can do active case finding, searching for cases that might have been missed.
The next step is to talk to people. The disease detective’s most important tool is conversation. The work requires patience, empathy, and absolute confidentiality. In these types of investigations, people will tell you who they kissed, who they slept with, who they shared a needle with . . . but only if they trust you absolutely. The Hondius investigation required teams to ask elderly cruise passengers, in several languages, who they had been close to over a five-week voyage.
After that comes contact tracing. Sexually transmitted disease investigators, the most skilled interviewers in public health, can elicit the names of contacts from a rock. On the Hondius, that meant the passengers who disembarked at St. Helena, the dozens more on the Airlink flight from St. Helena to Johannesburg, and the KLM flight the widow boarded briefly and former passengers across more than twenty countries. Each gets a phone call and personal visit if possible, a temperature log, and a 42-day clock that started the moment they left the ship.
Cruise ships are basically petri dishes. People are packed together, ventilation is poor, and everyone touches the same surfaces. These are literally close quarters. Disease detectives have documented dozens of outbreaks on cruise ships over the years, from diarrheal disease, to respiratory disease, and even tuberculosis. So it’s not surprising this strain of hantavirus spread once it boarded. On a cruise ship like the Hondius, that means everyone on board is a high-risk contact.
Quarantine is what you do with people who might be infected but aren’t yet sick. It’s been a tool of public health since the Ragusan trentina of 1377—thirty days off the coast of plague-stricken ships, soon extended to the forty-day quarantena, the source of the word. Hold a possibly infected person away from others until symptoms appear and you prevent a chain from forming.
Isolation is different. It’s for people who are sick and potentially infectious. Quarantine separates the well-but-exposed; isolation separates the ill. On the Hondius, the sequence was: identify the sick, isolate them, identify the exposed, quarantine them, and care for the sick to maximize survival.
Hantavirus includes a wide range of viruses, with more than 50 species, and many subtypes within those. The 1993 Four Corners outbreak of Sin Nombre virus killed 27 Americans nationwide, more than half of those it infected. The Andes strain is different. It’s the only hantavirus we know of that’s both deadly and able to spread from one person to another. There is no antiviral treatment and no proven vaccine, but that doesn’t mean there’s nothing doctors can do. Intensive care—oxygen support, fluid management, extracorporeal membrane oxygenation (ECMO), mechanical ventilation when needed—can turn an often fatal disease into a survivable one. One British passenger, evacuated from Ascension Island to Johannesburg, is struggling in the ICU but, as of this writing, still alive.
The work of disease detectives comes down to two cardinal principles: minimize spread, maximize survival. Assess, isolate, treat intensively, and quarantine. Monitor quarantined people daily. If one falls ill, isolate, assess, and treat—fast. Patients with the Andes virus can go downhill quickly.
Disease detectives are usually invisible. It’s patient, quiet, methodical work, and it saves more lives than almost any other profession. The Hondius outbreak will end sooner because dozens of them did this work well. Disease detectives live to stop outbreaks like this one. Support them—and their institutions, including CDC—and we can all breathe more freely and live longer..
To learn more about disease detectives, I hope you’ll read The Formula for Better Health: How to Save Millions of Lives Including Your Own.